When learning basic and advanced electrocardiography, sometimes the best place to start is a whiteboard.
 |
| Figure 1: A simple line-art rendering of the conduction system of the heart, divided into the atria and ventricles. Present are the sinoatrial node, internodal pathways, Bachmann's Bundle, atrioventricular node, Bundle of His, right and left bundle branches. Absent are the Purkinje fibres, valves, atrial and ventricular septa, and great vessels. |
From the basic "conduction road map" of the heart, seen in
Figure 1, we can start illustrating concepts.
 |
| Figure 2: The sinoatrial node depolarizes and the depolarization wavefront travels rapidly along the internodal pathways and Bachmann's Bundle, towards the atrioventricular node and the left atrium. |
 |
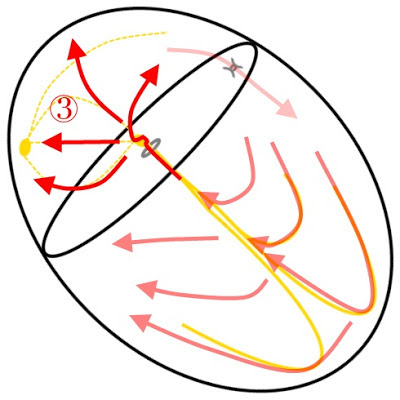
| Figure 3: As the atrial tissue repolarizes, the depolarization wavefront slows as it travels through the atrioventricular junction. This allows atrial systole to efficiently fill the ventricles. Once through the atrioventricular node the depolarization wavefront rapidly moves through the Bundle of His. |
 |
| Figure 4: Atrial tissue has almost completely repolarized and the tissues in the atrioventricular junction are beginning their repolarization. The depolarization wavefront now spreads rapidly through the right and left bundle branches and into the Purkinje System. |
Beginning in
Figure 2 and continuing through
Figure 4, we can see the propagation of a depolarization wavefront started in the sinoatrial node and its eventual path through to the bundle branches. While difficult to express on an actual whiteboard, fading of the older impulses is used to help represent the
time component of the signal.
Reentrant Tachycardias
The beauty of this style of drawing is the ability to convey concepts such as
Atrioventricular Nodal Reentry Tachycardia (
AVNRT). A certain subset of the population has two or more distinct zones of conduction in their AV node. Often there are dual pathways with one of the zones conducting impulses quickly but recovering slowly, and the other conducting impulses slowly and recovering quickly.
In a sinus rhythm this difference in conduction through the atrioventricular node is not apparent. However, if a well timed premature atrial contraction (PAC) is present, this dichotomy can be exploited. In
Figure 5 we can see the sinus impulse arriving at the AV node, with part of the wavefront traveling through the fast pathway, and part of the wavefront traveling through the slow pathway.
 |
| Figure 5: A sinus wavefront enters an atrioventricular node featuring dual pathways; a slow pathway which recovers quickly, and a fast pathway which recovers slowly. Barring outside influence, the presence of dual pathways itself does not initiate a tachycardia. |
Continuing in
Figure 6, the slow pathway with its shorter effective refractory period, begins recovering quicker than the fast pathway. Once through the AV node the depolarization wavefront continues through the Bundle of His and into the bundle branches and Purkinje fibres as during normal conduction.
 |
| Figure 6: The dichotomy of recovery in the two atrioventricular nodal pathways are illustrated. |
It is at this vulnerable point that a well timed extrasystole can take advantage of the heterogeneous repolarization of the AV nodal pathways.
Figure 7 depicts the initiation of a PAC which reaches the slow pathway while it is completely recovered and the fast pathway is still absolutely refractory.
 |
| Figure 7: An appropriately timed premature atrial contraction depolarizes the atrial tissue and arrives at the atrioventricular node as the slow pathway completes recovery. At this time of repolarization the fast pathway remains absolutely refractory. |
In
Figure 8 we can see the "rotation" of reentry initiated as the depolarization wavefront travels forward (
antegrade) through the slow pathway and backwards up (
retrograde) the fast pathway which has now recovered. Impulses are then distributed down through the Bundle of His each time the rotation through the slow pathway reaches the insertion of the Bundle of His. It is this reentry, best illustrated as a rotation, that not only initiates the tachycardia but sustains the tachycardia as well.
 |
| Figure 8: As the impulse from the PAC travels through the slow pathway, reentry of the fast pathway occurs when the impulse reaches the insertion of the Bundle of His. In the time it took the impulse to reach the Bundle of His along the slow pathway, the fast pathway had completed recovery, allowing retrograde conduction. The heterogeneous recovery rates of the two tissues allows the "rotation around" the AV nodal pathways, initiating and sustaining the tachycardia. |
When viewing
Figure 8, you may see why typical AVNRT results in a
Pseudo-S wave in Lead II (
Figure 9) and
Pseudo-R' wave in Lead V1, as once the tachycardia begins the impulses are conducted to the atria retrogradely from the fast pathway. Ventricular depolarization continues as it would during normal conduction, using the normal ventricular conduction tissues for propagation.
 |
| Figure 9: The Pseudo-S wave, highlighted in red, seen during typical atrioventricular nodal reentry tachycardia as the atria are depolarized retrogradely. |
Reentry Outside the AV Node
Atrioventricular nodal reentry is not the only means of reentrant tachycardias. Less than 1% of the population features an extra "exit" in their conduction road map, known as an
Accessory Pathway (
AP, featured in
Figure 10) or an
Accessory Bypass Tract.
Drs. Wolff, Parkinson, and White were the first to describe a series of patients featuring bundle branch blocks and a short PR intervals who suffered from paroxysms of tachycardias in the 1930's. However, it was not until the late 1940's that these abnormalities were isolated by Drs. Ohnell and Wood as bundles of conducting tissue which connected the atria and ventricles, independent of the AV node.
 |
| Figure 10: An example Accessory Pathway (AP) is illustrated on the ECG as another "hole" through the atrioventricular septum. AP's have been found along nearly every aspect of the atrioventricular septum and algorithms exist to classify their location based on changes seen on the surface ECG. |
AV nodal tissue features the property of decremental conduction; simply stated, it acts as a speed bump slowing the conduction of a depolarization wavefront. The upper limit of atrioventricular conduction is often less than 220 bpm although this varies with age. Typical accessory bypass tracts do not feature decremental conduction and can often conduct both antegrade and retrograde signals in excess of 220 bpm.
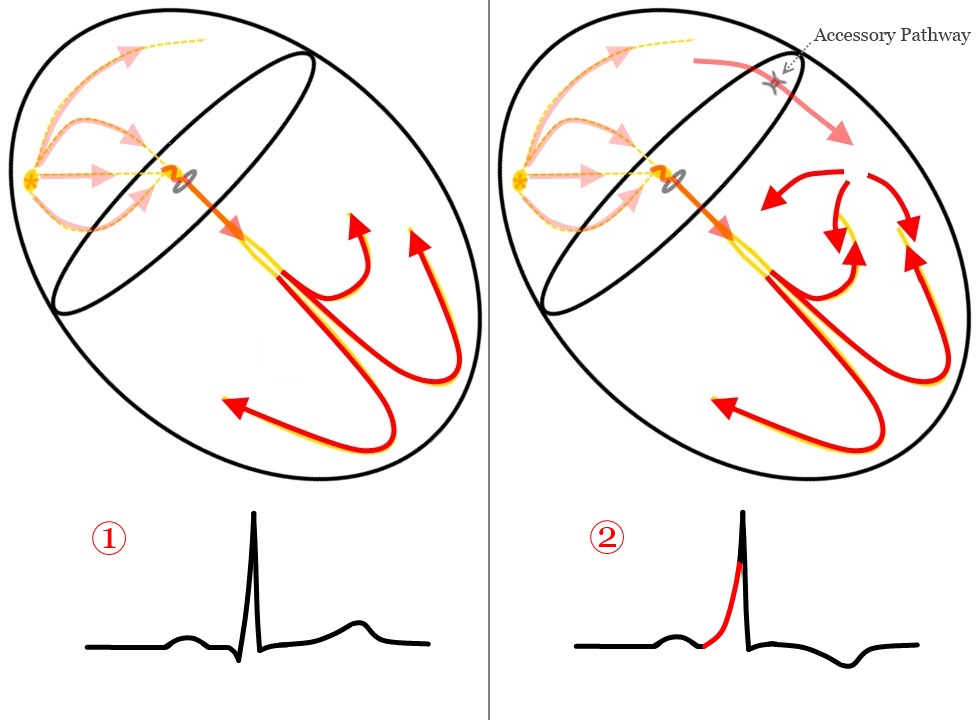
The hallmark feature of an AP is pre-excitation of the ventricles. As sinus impulses arrive at both the AV node and the AP, illustrated in
Figure 11 and
Figure 12, the depolarization wavefront is slowed in the AV node but conducted without delay through the AP.
 |
| Figure 11: A sinoatrial node depolarization travels towards the AV node and an Accessory Pathway (AP). |
Figure 12 shows that ventricular myocardium begins depolarizing as the AP terminates directly into ventricular tissue.
 |
| Figure 12: The depolarization wavefront is conducted through both the AV node and the AP. However, the AP conducts the impulse without delay and begins depolarization of a portion of the ventricle not a part of the normal conduction network. |
In
Figure 13, this direct connection to ventricles
pre-excites some myocardium while normal conduction through the bundle branches from the AV node occurs.
 |
| Figure 13: As depolarization of the ventricles continues, the two wavefronts meet. The fusion of these two wavefronts often mimics a bundle branch block. |
Fusion of the normal and pre-excited wavefronts produce the characteristic
Delta Wave of WPW in
Figure 14a and
Figure 14b.
 |
| Figure 14a: Comparison of the QRS morphology during a sinus rhythm and a sinus rhythm with pre-excitation through an accessory pathway. |
 |
| Figure 14b: As the depolarization wavefront travels through the AV node and AP, it reaches the ventricular myocardium faster through the AP. This results in depolarization of some tissue before it would normally occur if initiated through the bundle branches and Purkinje Fibres. This pre-excitation is seen on the surface ECG as a perceived shortening of the PR interval and the characteristic (1) slurring of the intrinsicoid deflection known as a Delta Wave. This heterogeneous depolarization results in a different order of repolarization typically manifests itself as (2) abnormal ST/T-wave changes. |
Reentry Using an Accessory Pathway
If pre-excitation were the only feature of an accessory pathway, Wolff-Parkinson-White would exist merely as a fascinoma. However, as previously noted, most accessory pathways are pathological featuring non-decremental antegrade and retrograde conduction.
This additional circuit may join with the AV node and be exploited by extrasystoles or heterogeneous repolarization. This class of tachycardias is known as
Atrioventricular Reciprocating Tachycardia (
AVRT) or the older Circus Motion Tachycardia (CMT).
Orthodromic Reentry
AVRT is divided into two types based on the direction of travel in the circuit.
Orthodromic AVRT occurs when the reentry is antegrade through the AV node then retrograde through the AP; thus conduction through the ventricles proceeds normally. An orthodromic circuit can be initiated by a premature ventricular contraction (PVC) or blocked antegrade conduction through the AP.
Figure 15 illustrates the arrival of a sinoatrial depolarization at both the AV node and the AP, with forward conduction through the AP blocked.
 |
| Figure 15: A sinoatrial depolarization arrives at the atrioventricular node and an accessory pathway, finding the AP blocked. |
While antegrade conduction is blocked at the AP, it is not at the AV node and ventricular depolarization begins normally in
Figure 16.
 |
| Figure 16: Conduction proceeds normally through the AV node. |
However, as ventricular depolarization continues it finds the AP to be available for retrograde conduction in
Figure 17.
 |
| Figure 17: As the ventricles depolarize and conduction continues through the ventricles the wavefront finds that retrograde conduction through the AP is not blocked, contrary to antegrade conduction. |
Figure 18 continues as the ventricular depolarization wavefront returns to the atria retrogradely through the AP. Depolarization of the atria occurs and the wavefront reaches the AV node. An orthodromic AVRT is then initiated and sustained as the wavefront continues antegrade through the AV node and into the ventricles, using the AP to return retrogradely to the atria.
 |
| Figure 18: The ventricular depolarization wavefront continues retrograde through the AP into the atria, arriving back at the AV node. At this point the Orthodromic AVRT circuit can begin, continuing through the AV node. The tachycardia is sustained as impulses use the AP retrogradely and the AV node antegradely. |
As with AVNRT, orthodromic AVRT uses the normal ventricular conduction network and features rapid propagation of ventricular depolarization visualized as narrow QRS complexes. Retrograde atrial activation may or may not produce visible P-waves on the surface ECG, depending on the location of the AP.
Antidromic Reentry
In
Antidromic AVRT, conduction of the reentry circuit begins antegradely through the accessory pathway and completes retrogradely through the atrioventricular node. Because ventricular depolarization does not begin with the normal ventricular conduction network, antidromic AVRT will present as a regular wide complex tachycardia due to slower propagation of ventricular depolarization.
As in orthodromic AVRT, an antidromic circuit can begin with an extrasystole or with blocked conduction. In
Figure 19, a PAC travels forward through the atria entering an accessory pathway and is concurrently blocked by a refractory AV node.
 |
| Figure 19: An atrial extrasystole finds the AV node refractory, however, is able to conduct antegrade through an accessory pathway into the ventricles. |
Depolarization of the ventricles begins outside the conduction network, in the myocardium, and propagates slower than in normal conduction in Figure 20.
 |
| Figure 20: Activation of the ventricular myocardium begins outside the conduction network and eventually reaches the AV node. |
Figure 21 continues with the ventricular depolarization entering the AV node retrogradely and depolarizating the atria.
 |
| Figure 21: Retrograde depolarization of the AV node and atria occurs. The accessory pathway does not feature the decremental conduction seen in the AV node and is already completely repolarized. |
In
Figure 22 the antidromic AVRT circuit is complete as the atrial depolarization wavefront continues antegrade through the AP and begins ventricular depolarization again.
 |
| Figure 22: The atrial depolarization wavefront continues antegradely through the AP and begins depolarization of the myocardium. At this point an Antidromic AVRT circuit is completed, featuring antegrade conduction through the AP and retrograde conduction through the AV Node. |
AVNRT and AVRT are generally well tolerated by patients as they both feature reentry through the AV node. The decremental conduction found in atrioventricular nodal tissue acts as a natural buffer for the reentry circuits keeping their rates less than 220 bpm and more typically less than 200 bpm.
Atrial Fibrillation and Wolff-Parkinson-White
Unfortunately, reentry rhythms are not the only means of tachycardias utilizing an accessory pathway. If an automatic atrial focus were to have access to a non-decremental accessory pathway the results will be rapidly fatal. Many patients with Wolff-Parkinson-White will experience episodes of atrial fibrillation (AF). In atrial fibrillation, numerous atrial wavefronts are present producing cyclic rates of 400-800 bpm.
Atrial fibrillation and WPW is characterized by varying degrees of fusion between antegrade conduction of f-waves through the AV node and the AP. This is seen on the surface ECG as a rapid, grossly irregular tachycardia with alternating QRS morphologies ranging from narrow to very wide.
Figure 23 features atrial fibrillation wavefronts depolarizing the AV node and encountering a refractory accessory pathway.
 |
| Figure 23: Atrial fibrillation with conduction through the AV node and blocked conduction through an AP. |
Conduction continues in
Figure 24 normally through the bundle branches and Purkinje Fibres. Conduction of atrial fibrillation in this manner will result in ventricular rates mediated by the decremental conduction of the AV node.
 |
| Figure 24: Conduction through the bundle branches and Purkinje Fibres propagates normally and the continued f-waves are blocked at both the refractory AV node and AP. |
Figure 25 highlights pathological, uninhibited conduction of the f-waves through an AP, propagating through the ventricular myocardium. As this AP features non-decremental conduction, f-waves are allowed to propagate as quickly as the ventricular myocardium can recover, often in excess of 260 bpm.
 |
| Figure 25: Non-decremental antegrade conduction of f-waves from atrial fibrillation through an AP into the ventricles. These f-waves are limited in propagation only by the effective refractory period of the AP and ventricular myocardium. |
As the AV node recovers, varying degrees of conduction through both the AV node and AP occur, resulting in fusion of ventricular depolarization wavefronts. Occasional decremental conduction through the AV node contributes to the grossly irregular ventricular rates seen in pre-excited atrial fibrillation.
 |
| Figure 26: Varying degrees of fusion occur as antegrade conduction proceeds through the AV node and AP. |
In Atrial Fibrillation with WPW, ventricular depolarization may reach rates close to 300 bpm and without intervention will degenerate into ventricular fibrillation.
I hope my digital reproductions of Whiteboard Cardiology proved useful and drop me a line if you have ideas for other concepts in electrocardiography that would be simplified through line art.
All of these images are free to use and licensed Creative Commons Attribution-Share Alike 3.0, available for download on my Google Drive. The originals were created using Paint.Net.


























13 comments:
This is fantastic! Understanding what happens and how it occurs makes it so much more easy to perform ECG interpretation than rogue pattern memorization. I especially like the slides that also featured ECG complexes. That brought it home. More,please!!!
Cardiology is subspecialty of internal medicine and a person who is planning to practice cardiology should go through residency program. cardiology residency length gives specialized practice and training. In the program, you will have the opportunity to learn about preventing, treating and diagnosing conditions and diseases of cardiovascular system and heart.
The gpa problems can overcome a low grade point average by compensating in other areas. The reasons for having a low GPA and the school you are applying to can also be a factor.
Business school essays will be discouraging, as candidates try and decide what to write down regarding and the way to best convey their experiences and enthusiasm to the master's degree admissions committee. internship motivation
The abilities of the doctor of this hospital are unbelievable and working so hard. The transplant is one of the difficult things and you have to examine every part of the body but sample eras application provides nice job. Helen is under the process of the transplant and doctors are working so well.
Good day I am so glad I found your website, I really found you by error, while I was browsing on Bing for something else, Anyhow I am here now and would just like to say thanks a lot for a fantastic post and a all round thrilling blog (I also love the theme/design), I don’t have time to read through it all at the minute but I have bookmarked it and also added in your RSS feeds, so when I have time I will be back to read a lot more, Please do keep up the awesome work. find a cardiologist in london
Learning electrocardiography is explained with white board method is really easy to study. Consult good cardiologist near you in cardiac difficulties.
nice information.Doctoriduniya
Nice explanation about white board cardiology.
Best Cardiologist London
well written health blog it is very informative , follow Meddco healthcare https://www.meddco.com/ for the best health treatments and and affordable diet plans
Thank you because you have been willing to share information with us. we will always appreciate all you have done here because I know you are very concerned with us.
Regards,
Cardiologist near me
Thank you for the insightful illustrations and explanations on electrocardiography. It’s fascinating to see how well concepts like AVNRT and accessory pathways are explained through visual depictions. For more information on heart conditions and treatments, you might find Dr. Manish Juneja’s work invaluable. His expertise in cardiology can offer further insights into heart health. Check out Dr. Manish Juneja for more details. Great content here!
Post a Comment